Podiatrist and Vascular Specialist Agree: Your Plantar Fasciitis Was Never a Foot Problem — It’s a Calf-Fascia Chain That’s Been Pulling on Your Heel for Years

Our readers at FootHealth.Life keep sending us the same photo. A tennis ball, a foam roller, an ice pack, and a night splint on the bedroom floor. And a single question. Why is my foot still killing me when I get out of bed?
It’s a fair question. They’ve been rolling the foot. Stretching the foot. Splinting the foot. Massaging the foot. Icing the foot. For months. Sometimes years.
So we reached out to two specialists. They’ve spent their careers on opposite sides of this problem.
Dr. James Caldwell, DPM — a board-certified podiatrist with 22 years in practice. And a vascular medicine researcher we consulted whose lab studies how blood reaches connective tissue. She asked not to be named while this article was being prepared.
The first thing both of them said, almost word for word, was this:
“The pain is in the foot. The problem isn’t. If you’ve been treating only what hurts, you’ve been treating the symptom for years. Your calf has been pulling on that fascia the entire time — and no one ever told you that’s where to look.”
“The plantar fascia doesn’t live in isolation,”1 the researcher adds. “It’s the bottom anchor of a chain that runs up through your Achilles into your calf. When the calf locks, the fascia gets pulled tight 24 hours a day — including the eight hours you’re asleep. That’s why the first step in the morning is the worst step. The calf has been pulling all night.”
We asked both specialists the same follow-up: if this has been known in the research for years, why is almost no one fixing the calf?
Their answer surprised us. It’s not that patients don’t try. It’s that almost every calf-targeted thing patients try — stretches, foam rolling, calf raises, even night splints — only addresses one piece of a four-piece problem.
3 facts about plantar fasciitis that explain why your foot-focused treatments keep failing
Both experts started with the science.
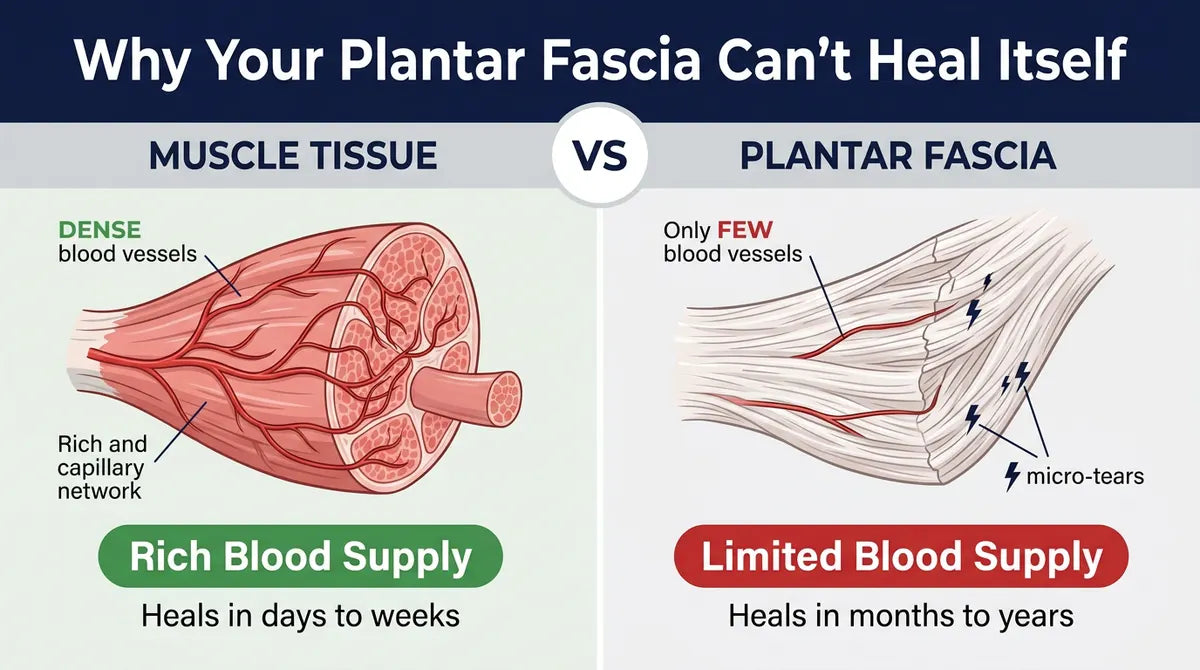
Fact #1: Your plantar fascia has almost no blood flowing through it
“The plantar fascia is a thick band of tissue. It’s dense. And it has barely any blood vessels running through it,”2 the researcher explains. “When a muscle gets damaged, your body sends blood to heal it. Your fascia doesn’t have that supply line.”
That matters. The tissue can’t heal at normal speed. Small damage piles up faster than it can repair. That’s why a condition that “looks simple on an MRI” is so hard to actually fix — and why icing it (which constricts blood flow even further) often makes things worse, not better.
Fact #2: The calf is the muscle that’s been guarding your fascia — without you ever choosing it
“This is the part almost nobody explains,” Dr. Caldwell says. “When your fascia hurts, your body recruits the closest large muscle to splint the area. For the plantar fascia, that muscle is the calf.”
“You don’t choose this. Your nervous system does it for you. It happened months or years ago — the first time the heel pain started. And the calf has been holding that protective tension ever since. Every step. Every night. Even when the heel isn’t actively hurting.”
“The problem is: a guarded calf squeezes the blood vessels that feed the fascia. The tissue that was already starved for blood gets even less. And the same calf, by being chronically shortened, pulls the fascia tight at the heel insertion point twenty-four hours a day. So every step lands on tissue that’s being yanked from above.”
That’s why standard calf stretches alone — the wall lean, the curb drop, the towel pull — rarely solve it. They lengthen the muscle for two minutes. The nervous system tightens it right back the moment you stop.
Fact #3: You can’t fix a four-point loop one point at a time
“Here’s the part that changes everything,” the researcher says.
“Plantar fasciitis isn’t a single injury. It’s a four-point loop. Pain signal. Calf guarding. Blocked blood flow. Starved tissue. Each one keeps the other three in place.”
Every treatment you’ve ever tried breaks exactly one of those four points. The other three put the loop right back within hours.
“You can’t pick a four-pin lock one pin at a time. For twenty years, that’s what we’ve been asking patients to do. Stretch the calf. Then ice the heel. Then wear a splint. Then roll a ball. The loop doesn’t open until you hit three points in the same session.”
Already recognize this pattern in your own treatment history?
Skip to the solution ›Score every calf and foot treatment you’ve ever tried against the 4-point loop
We asked Dr. Caldwell to walk us through the most common treatments — both the foot-focused ones AND the calf-focused ones patients eventually graduate to. One by one. Which point of the loop does each one actually break?
The pattern was striking.

“None of these are wrong,” Dr. Caldwell said when we showed him the table. “They all do something real. The calf stretch is genuinely useful — for the two minutes you’re doing it. The night splint holds the calf in a lengthened position — for the eight hours you’re asleep, at the cost of your sleep. But a four-point loop doesn’t open with a one-point fix. The math is right there.”
“This is why I’ve changed how I talk to patients. The question isn’t ‘which treatment is best.’ It’s ‘which combination releases the calf, restores blood flow to the fascia, and quiets the pain signal in the same session.’ Those are very different questions. And only one of them has a useful answer.”
If your own score would be 1 of 4 across every treatment you’ve tried — here’s the at-home protocol that hits three points at once.
Skip to the solution ›The three therapies that open the loop — clinicians call it “Hemodynamic Therapy”
“The research on fascia and the calf chain has been clear for more than twenty years,” the researcher says. “Three treatments, delivered in the same session, are what it takes to hold the loop open long enough for the tissue to start repairing.”
She gave us the name clinicians use for it informally: Hemodynamic Therapy.
It’s three things, at once:
1. Targeted heat (104–107°F). Opens the small blood vessels that feed the fascia and warms the calf tissue so it can release without fighting back. The supply line the tissue has been starved of.
2. Rhythmic compression. Pumps blood through the foot and lower calf the way a working muscle would. Because the fascia has no muscle pump of its own, you have to give it one from the outside.
3. Low-level neuromuscular activation. Gentle electrical pulses release the guarding calf muscle at the source — not just stretch it for two minutes. So it stops squeezing the blood vessels shut and stops pulling on the fascia.
“One alone doesn’t work. Two doesn’t. Three at once is the threshold. The fourth point — the pain signal — quiets on its own. Because nothing is holding it active anymore,” the researcher says.
“And critically: this is what a night splint can’t do. A splint holds position. It doesn’t release the calf. It doesn’t move blood. It doesn’t quiet the pain signal. It addresses a fifth thing — overnight tissue position — while doing nothing about the four things that actually matter.”
Hemodynamic Therapy — all three therapies, delivered in a single 15–20 minute at-home session before bed. No splint required.
Skip to the solution ›What Mayo Clinic, Johns Hopkins, and others have published — and why this is finally reaching patients
The three-therapy combination isn’t new in the research world.
Research groups at institutions like Mayo Clinic, Johns Hopkins, and the American College of Sports Medicine have published extensively on multimodal soft-tissue recovery over the past decade. They’ve documented how heat, compression, and electrical stimulation work together to restore blood flow and release guarding muscles in connective tissues like the plantar fascia and the calf chain that feeds into it.
Until recently, though, you could only get all three together in a clinic.
Two to three visits a week. $150 to $250 per session. Plus the insurance pre-approvals that most people never cleared.
“Most of my patients couldn’t do that — financially, logistically, or because the foot that already hurt was the same foot they’d need to drive with,” Dr. Caldwell says. “So they settled for one therapy at a time. Which is exactly why the loop never opened.”
That has started to change.
Over the last 18 months, a small number of companies have commercialized Hemodynamic Therapy for at-home use — designed around the same three-therapy combination clinicians have been using for years. One of them agreed to offer our FootHealth.Life readers a direct rate, without the typical clinic markup.
A reader-secured direct rate: the Soleus Foot Therapy System

The device FootHealth.Life readers have written in about most is called the Soleus Foot Therapy System. It’s a simple neoprene wrap that delivers all three parts of Hemodynamic Therapy — targeted heat, rhythmic compression, and low-level neuromuscular activation — in one short session that releases the calf, moves blood through the fascia, and quiets the pain signal at the same time.
No clinic. No appointment. No driving. No plastic strapped to your shin all night.
- Strap it around your foot and lower calf, press one button, run for 15–20 minutes
- All three Hemodynamic Therapy modalities run together in the same session
- Worn lying in bed before you sleep — then taken off. You sleep normally.
- Cordless and rechargeable — use it anywhere at home
It’s not a prescription device. It’s a wellness product built around the same three-part combination clinic sessions use. Whether it’s right for you depends on your situation. But if you’ve been cycling through single-point treatments — foot-focused or calf-focused — it’s at least worth reading the details.
See the reader rate ›What patients who’ve used it are reporting
“Three doctors told me I just had to live with it. I spent five years and more than six thousand dollars trying to prove them wrong. After two weeks using it I went from bracing on the bathroom counter every morning to just standing up. Last Saturday I walked the farmers market for two hours without sitting down. I kept waiting for it to be a fluke. It wasn’t.”
“I had two cortisone shots this year. My podiatrist said no more. I figured I was out of options. My daughter pushed me to try this. About three weeks in, my husband noticed before I did — he said ‘you used to wince when you stood up.’ I hadn’t realized I’d stopped.”
“I’m a nurse, on my feet all day. PT, orthotics, night splint — none of it held. This is the first thing that actually changed my mornings. I use it while I watch the news before bed. Simplest thing in the world.”
*Testimonials reflect the experiences of individual users. Individual results may vary. These are not guaranteed outcomes and are not intended as medical advice.

The takeaway
Both specialists we spoke with landed on the same point.
Plantar fasciitis doesn’t fail to resolve because patients haven’t tried hard enough. It fails because the pain is in the foot but the cause runs through the calf — and single-point treatments, no matter how good, can’t hold that loop open long enough for the tissue to repair.
“If you’ve been stuck in the cycle, I’d encourage you to look at options that hit multiple points of the loop at once,” Dr. Caldwell said at the end of our call. “Not because any device is a guarantee. But because the math of the loop is real. And the calf isn’t going to release itself.”
Whether it’s a clinic program, an at-home device like Soleus, or something else — the category is what matters.
The era of “just stretch your calf and wear the splint” may finally be ending. Not because the treatments got better. Because we finally started counting how many points of the loop we were breaking at once — and stopped pretending the foot was where the problem began.
References
- American Academy of Orthopaedic Surgeons — “Plantar Fasciitis and Bone Spurs” (OrthoInfo).
- Martin R.L. et al. — “Heel Pain — Plantar Fasciitis: Revision 2014.” Journal of Orthopaedic & Sports Physical Therapy Clinical Practice Guideline.
- Cleveland Clinic — “Plantar Fasciitis: Symptoms, Causes & Treatment.”
- Mayo Clinic — “Plantar Fasciitis: Symptoms and Causes.”